Written by Dr Ryan Lee, Consultant obstetrician and Gynaecologist Specialist
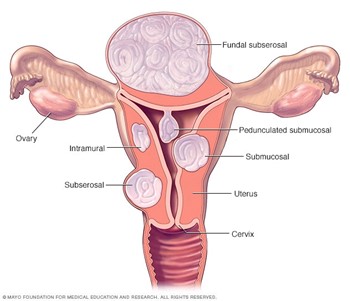
Fibroids or leiomyoma are growths of the uterus (womb). Fibroids are very common affecting about 30-60 percent of females having fibroids in their lifetime. The locations of fibroids vary in the uterus below.
Risk factors
Unfortunately, about 5 % will have bothersome symptoms such as pressure symptoms, urinary or bowel difficulties, menstrual problems like painful and/or heavy menses or difficulty getting pregnant. Fibroids are usually not cancerous with a less than 1% risk of becoming cancer known as leiomyosarcoma.
The cause of fibroids is unknown. However, fibroids seem to respond to the female hormones’ oestrogen and progesterone. It is possible for a person without any known risk factors to develop fibroids. Other factors which may increase your risk for developing fibroids are:
- Family history of fibroids like your mother or sister
- Diet high in red meat and low in vegetables, fruit and dairy products
- Obesity
- Alcohol consumption
Hence, maintaining a healthy lifestyle and weight can reduce a woman’s risk of developing fibroids.
Symptoms
The majority of fibroids are small and do not cause any symptoms at all. Fibroids are more likely to cause symptoms if the fibroids are large> 5 cm, multiple number of fibroids and/or if the fibroid is located in certain places in the uterus. Fibroid symptoms tend to get better during the menopause.
Symptoms of fibroid include the following below
-Heavy menstrual bleeding — Fibroids can increase the amount and/or the number of days of menstrual bleeding. People who have excessive menstrual bleeding are at risk of losing too much iron and suffer from iron deficiency anaemia.
-Pelvic pressure and pain — Larger fibroids can cause a sense of pelvic pressure or fullness in the abdomen, similar to the feeling of being pregnant.
-Urinary symptoms like urinary retention of urine or bowel constipation if the location of the fibroid is near the bladder or the rectum respectively
– Difficulty getting pregnant especially if submucosal fibroids or intramural fibroids are distorting the inside of the uterus,
-Most women with fibroids have a completely normal pregnancy without complications. However, women with large fibroids (greater than 5 cm or multiple fibroids might have an increased risk of specific pregnancy complications such as increased risk of miscarriage, preterm labour and abnormal lie/fetal presentation and requiring a caesarean section.
Diagnosis
Diagnosis of fibroid is made by clinical examination and ultrasound pelvis scan. On clinical examination, your uterus may be found to be enlarge when feeling for a mass in the abdomen. A pelvic ultrasound can then be performed to confirm the presence of fibroids

Treatment
There are many treatments for fibroids, and it can be hard to decide which one is right. You should choose a treatment based upon your fibroid-related symptoms and whether or not you might want to get pregnant in the future. The best treatment options depend on which symptom(s) is most bothersome. The size, number, and locations of fibroids and desire for fertility are factored into treatment decisions.
If your fibroids are not causing bothersome symptoms, you can opt for no treatment with conservative treatment. If you do have symptoms, your options include medication or surgical treatment.
If you are bothered by heavy menstrual bleeding, you can first try medications. Hormonal birth control, nonsteroidal anti-inflammatory drugs (NSAIDs), or antifibrinolytic medicines are suitable first line treatment options.
If medication is not a good option for you, or you also have symptoms related to the size of the fibroids, you can consider surgical options like myomectomy or hysterectomy.
Uterine fibroid embolization, focused ultrasound surgery may be considered as alternative for patients who decline surgery or don’t respond to oral medications.
Medications
Most medications aim to reduce the heavy menstrual bleeding and/or period pains.
Antifibrinolytic medication such as tranexamic acid (Cyklokapron) do not contain hormones and can help to slow menstrual bleeding quickly. They work by helping blood to clot. Antifibrinolytic medications do not shrink fibroids or correct anaemia.
Nonsteroidal anti-inflammatory drugs (NSAIDs) such as mefenamic acid/naproxen which can also be used to reduce menstrual cramps and decrease heavy menses.
Iron tablets can be taken to treat iron deficiency anaemia.
Side effects can include headache and muscle cramps or pain. You should not take antifibrinolytic medications with hormonal birth control unless your doctor or nurse approves; there may be an increased risk of blood clots, stroke, and heart attack when taken together.
Injectable medications like GnRH analogues like Lucrin can be given to reduce the size of the fibroid and stop menstruation temporally for up to 6 months, however the fibroid will likely grow back after the injection is stopped.
Intra-uterine device (IUDs) slowly release a form of a progesterone-like hormone into the uterus. There is no estrogen in the IUDs. The 52 mg levonorgestrel-releasing IUD (Mirena) has been studied the most for the treatment of heavy menstrual bleeding which have been found to be highly effective.
Surgery
Surgery is indicated over medications in women
– Not responding respond to medications
– suffering from pressure symptoms such as urinary or bowel problems
– Those trying to get pregnant with fibroid affecting the womb cavity
– Large size of the fibroid causing pressure symptoms
– decline medications
Type of surgery
1.Myomectomy — Myomectomy is a surgery done to remove fibroids, which can reduce both bleeding and size-related symptoms. However, there are some risks:
Fibroids can come back after myomectomy. Between 10 and 25 percent of people who have myomectomy will need a second fibroid surgery. While rare, some people will need to have a hysterectomy while undergoing myomectomy due to massive blood loss and hysterectomy is a permanent surgery that removes the uterus instead. Women are advised to delay pregnancy for a minimum of 6 months after myomectomy and may require a caesarean section for large fibroids removed that breach the endometrial cavity during myomectomy to reduce the risk of uterine rupture.
There are several ways to perform myomectomy; the type of myomectomy depends on location and the size and number of fibroids.
Abdominal myomectomy – This surgery requires a cut in the lower belly to remove the fibroids by open surgery
Vaginal hysterectomy removes the uterus through the vagina. This is suitable for those with smaller fibroids.
Laparoscopic myomectomy – This is a form of minimal invasive surgery that several small incisions and the fibroid removed through by cutting it into smaller pieces for removal (morcellation)

Transcervical resection of myoma ( TCRM)– is performed for fibroids inside the uterus for submucosal fibroids by hysteroscopic method.

2. Hysterectomy is a permanent treatment that cures heavy menstrual bleeding and the bulk of related symptoms of fibroids. After a hysterectomy, a person will not be able to get pregnant and have no more menses. It is recommended in women who have no child bearing wishes, completed family, multiple large fibroids or have yet previous myomectomy.

Alternatives
Several alternatives are available in addition to medication and surgery.
Uterine artery embolization — a treatment that blocks the blood supply to fibroids. This causes the fibroid to shrink within weeks to several months after the treatment and decreases other fibroid symptoms including heavy menstrual bleeding. Pregnancy is not usually recommended after uterine artery embolization.
Endometrial ablation and resection involves removing the lining of the uterus.
Magnetic resonance-guided focused ultrasound — Magnetic resonance-guided focused ultrasound surgery (MRgFUS or FUS). This non-invasive treatment uses ultrasound energy which leads to thermal destruction of the fibroid and takes place in an MRI machine.
Summary
Fibroids are muscle cells that grow in and around the womb. The cause of fibroids is unknown. Your health care provider may find fibroids during a gyanecological exam or by pelvic ultrasound. Treatment includes drugs that can treat symptoms or surgery such as myomectomy or hysterectomy. Many women with fibroids can get pregnant naturally, however they are more likely to require a caesarean section after fibroid surgery. Ultrasound surveillance is recommended in patients with fibroids having symptoms to monitor fibroid size and evaluate treatment options.